Anal abscess and fistula
Anal abscess and fistula
Anal abscess and fistula is a frequent disease that causes inflammation in the anus, pain, swellings and fluid discharge. It is characterized and caused by an opening inside the anal canal. Treatment of anal abscess- fistula is at times difficult and inflammation can sometimes reappear.
Fistula or abscess?
Perianal abscess is a collection of pus around anal canal. This acute condition is characterized by pain, and local inflammation, rarely with fever while fistula is a long-standing, relatively painless lesion with pus discharge. Flare-ups and remissions are quite common in perianal abscesses. Pus and inflammation should be treated as an emergency by surgical drainage of pus. Postoperatively, a skin opening with pus discharge is left (a perianal fistula) at the site of surgical incision.
Causes of perianal inflammation
Perianal inflammation is caused by an infection expanding from an internal anal opening. In case of hidradenitis (skin disease), there is no intra-anal opening. Hidradenitis is more frequent in obese and smokers. Rarely, anal fistulas are a manifestation of Crohn’s disease or after external blunt injury or foreign body ingestion. Other uncommon types of anal fistula are postoperative fistulas, fistulas after pouch surgery, low anterior resection, anovaginal or rectoprostatic fistulas.
Symptoms
Abscesses appear quickly within a few days as a painful inflamed swelling, occasionally with fever. Fistulas appear as an opening with pus discharge. Skin openings may heal or reappear. In case, there are multiple skin openings and fistulas, hydradenitis maybe suspected. Rarely, fistulas can be early diagnosed only with the presence of a painful intra-anal bulge.
Diagnosis and preoperative diagnosis
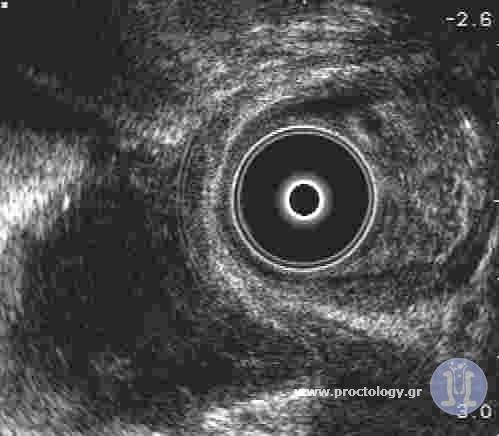
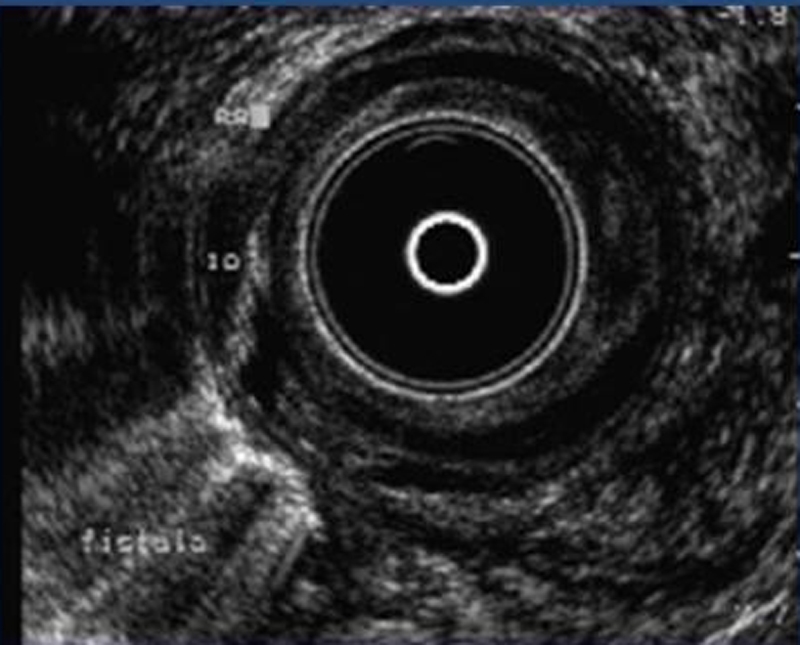
An important feature in the diagnostic and therapeutical assessment of perianal fistulas is the exact location of internal opening in the anal canal. Other significant features of preoperative assessment are fistula’s position in correlation with the anal sphincters (circular muscles around anus which keep stools inside anal canal) and the proportion of sphincters’ muscle beneath the fistula tract. Manual examination by an experienced surgeon may provide significant information about orientation of fistula. For the diagnostic assestement of perianal conditions is frequently a NMR scan (Nuclear magnetic resonance) is performed. However, in our practice, we have been using 3d endoanal ultrasound for 25 years. Due to our long-term experience with 3d ultrasound, we are able to obtain an immediate diagnosis and detailed information in mm about significant features of fistula tract and its relationship to anal sphincters. On the contrary, NMR usually gives indefinite answers to the above questions and even completely wrong information, in the worst of cases.
Treatment Techniques (laser)
Abscesses containing pus should be treated incising the abscess cavity and draining pus. If the surgery is delayed, abscesses can get worse and the patient may have quite important pain. In rare occations, septicemia with hypotension may also occur. Small abscesses can be incised with local anesthesia after a detailed mapping with ultrasound. If abscesses are not eventually surgically drained, they grow significantly and penetrate deep into anal sphincters, complicating ] treatment. Because abscesses usually originate from a intra-anal opening, after operation a fistula appears with pus discharge at the site of incision. This condition is usually treated later. Fistula (internal opening) occurs before the emergence of abscess. Abscesses can be described as the tip of an iceberg (fistula). Therefore, the belief that poor drainage of abscess results in a fistula is totally wrong. In selected cases, full treatment of anal fistula-abscess can be achieved in single surgical procedure after a detailed 3d ultrasound assessment.
Antibiotics are prescribed in perianal abscess when an untrained surgeon cannot detect the abscess, especially if there is no preoperative diagnostic assessment. Antibiotics don’t heal fistulas completely, they only reduce inflammation temporarily, but the abscess often recurs.
There are more than ten available techniques for fistula treatment. The existence of various surgical techniques indicate that no technique is appropriate for all fistula cases. The main aim of the treatment is at first to preserve anal sphincters and secondarily to definitely treat fistula with the smallest wound and the less postoperative disablement.
Recently a lot of novel procedures (LIFT, Flap) and appliances (AFP, Permacol, VAAFT, OTSC, etc.) have been proposed for fistula treatment. The recent appliances have been heavily advertised with important financial benefits to medical providers before the subsequent manifestation of quite significant recurrence rates and disadvantages.
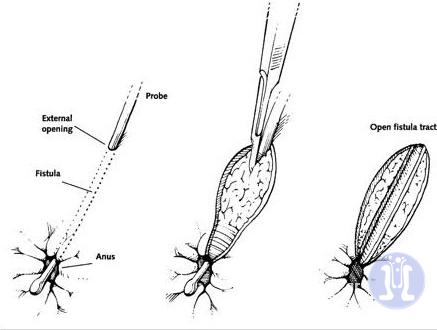
The oldest and simplest technique for treatment is laying open the fistula tract, that is to cut skin and other structures over fistula tract. This treatment is appropriate only for low fistulas not involving sphincters.
The use of a seton (loose or cutting) suture for more difficult fistulas has been used since ancient Greeks. But nowadays it has been substituted with LIFT or Mucosal flap procedures which don’t harm anal sphincters. LIFT or Mucosal flap techniques treat fistulas closing anal internal opening and preventing contamination. They are quite technically difficult, they are performed only by experienced proctologist surgeons and have a failure rate of around 30%.
In certain cases Filac-Laser technique is a promising technique because it does causes minimal injury to the structures and sphincters. Its success rate, according to the originator of the method, is about 60-70%.
Any proctologist surgeon operating fistulas should be able to perform all techniques but select the appropriate procedure in each patient. For a particular fistula surgery, we may use a combination of two or more techniques in order to obtain the best result. Some fistulas can be treated definitively with local anesthesia within half an hour. Complicated fistulas require patience and more than one surgical procedure. If both the patient and the surgeon establish bilateral trust between them, a definitive treatment is probable.
Postoperative course
Most fistula operations leave a wound with serous discharge. It heals evenly after proper wound care and frequent dressings. After laser surgery, the wound is minimal and the patient can return to his activities in a few days.
FAQs
Why preoperative diagnostic mapping of fistulas is necessary before any surgical treatment?
Preoperative mapping of anal inflammation provides a clear diagnosis about the location of fistula, its realtion with muscles and its origin (internal opening). This diagnosis is even more important in women who have shorter muscles which may be lightly damaged from birth. The examination is necessary in cases of incomplete treatment and reappearance of fistulas. Surgical treatment of fistulas is safe after a detailed ulktarsonic mapping of sphincters. Postoperative fecal incontinence is prevented after a detailed diagnosis.
What are the possible complications of fistula surgery?;
If the origin of the fistula (internal opening) or its branches are not treated, the fistula may reappear. If the anal muscles are cut during the operation, the patient may not hold his stools successfully.
Which is the treatment of simple – low fistulas?
Fistulas that are not related with anal muscles are successfully treated with a simple incision. A preoperative mapping with ultrasound is necessary to perform such an operation without any danger of sphincter damage and fecal incontinence. Simple fistulas can be treated with local anesthesia in the office without general anesthesia.
Which is the treatment of high fistulas
The fistulas that are related with anal muscles should be treated with more demanding operations (LIFT or mucosal flap). The simple laying open of high fistulas can result in fecal incontinence because there may be damage to anal muscles.
Does anal inflammation reappear?
Anal inflammation usually is caused by an opening inside anal canal. If this is not dealt with successfully the anal abscess reappears. Anal inflammation caused by hidradenitis ( a skin disease) can reappear in another location after a successful operation.
RELATED ARTICLES
The causes of inflammation around anus
1. Perianal fistula. Perianal fistula is caused by contamination from…