Anal Warts (HPV)
Anal Warts (HPV)
What are anal warts (HPV)?
Warts are small raised or flat swellings located in the genital area and the anus. They are caused by human papilloma virus (HPV) infection. HPV is usually transmitted through sexual intercourse. HPV may infect anus by direct sexual intercourse or indirectly with contaminated hands or sexual toys. There are around 40 HPV types. They cause warts, cancer and precancerous dysplasias in female external genitalia, penis, anus, mouth and tonsils.
The frequency of anal HPV infection in women is 70% and 24% in straight men. The frequency of anal HPV infection is 60% in gay and 90% in HIV seropositive gay people. Condom use is mandatory during anal intercourse for preventing infection but this protection is not complete.
HPV infection is not limited to the skin around anus only but also inside anal canal. In the anal canal, HPV infects skin cells but cannot infect bowel cells. Therefore, HPV does not extend more than 5-7 cm from anal opening. In anal HPV infection internal anal canal should also be examined with high resolution anoscopy and acetic acid.
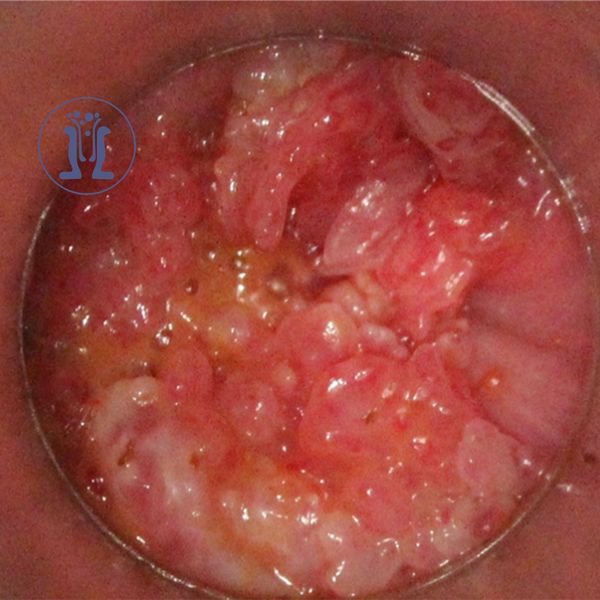
Anal warts are often perceived as small palpable nodules or because of itching. They can take the shape of lentils or cauliflowers, or they may involve large irregular surfaces. Perianal warts are easily diagnosed by direct eye examination and proctoscopy. Dysplasias that can progress to cancer cannot be diagnosed visually. the internal anal canal should also be examined with high resolution anoscopy and acetic acid.
Precancerous dysplasias do not cause any symptoms and cannot be easily detected because they are soft and flat. Acetic acid and high resolution anoscopy are necessary for their detection. Colonoscopy does not help for diagnosis of anal warts or dysplasias.
High-resolution proctoscopy should be performed in high-risk groups such as HIV-positive, immunodeficiency, anal intercourse, or female genital tract high grade dysplasias or cancer. Dysplasias can be detected also with anal cytology- pap-test (with a significant percentage of false negative results) and HPV test.
HPV infection, anal warts, anal dysplasias and anal cancer are more common in people who have had anal intercourse or more than 15 sexual partners. 15% of anal high-grade dysplasias progress to anal cancer. Anal cancer is more frequent in women with external genital cancer or dysplasias. Weak immune system is also a very important risk factor for development of anal warts, dysplasias or cancer.
Weak immune system occurs in HIV infection, in long-term treatment with steroids or other medications in transplanted patients, autoimmune disease or inflammatory bowel disease. Smoking intensifies HPV infection and facilitates its progression to cancer. Anal cancer frequency in gay is equal to cervical cancer frequency before the use of cervical cytology (test-pap).
Anal warts are treated with ablation, laser, cryotherapy or creams. Anal warts and dysplasias reappear frequently after any treatment. Therefore, a second examination 5-6 weeks post treatment is necessary. Steroid creams should be avoided because they weaken immune system and activate HPV.
A very important issue is HPV vaccination. The 9-valent HPV vaccine prevents 95% of HPV infections including most frequent HPV types and those types that cause cancer. HPV vaccination prevents anal cancer, cervix cancer and mouth cancer.
HPV vaccination is provided to men and women up to 26 years and up to 45 years in gay and HIV seropositive. HPv vaccination does not only prevent HPV infection but may also contribute to the treatment of already existing HPV infections (warts, dysplasias) by boosting humoral immunity beyond limited local cellular immunity induced by HPV infection.